Glubran® 2 in Thoracic Surgery
SURGICAL SPECIALIZATION
Seal. Protect. Heal.
Reducing Air Leaks and Improving Outcomes in Thoracic Surgery
Glubran® 2 is an aerostatic and hemostatic sealant designed for thoracic surgery. It provides suture reinforcement and ensures immediate aerostasis, supporting both manual and mechanical sutures. Its nebulized application creates a thin, elastic film that enhances tissue sealing while minimizing trauma.

Indications of Use
Glubran® 2 is indicated for:
- Sealing of bronchial and bronchopleural fistulas (diameter ≤ 6–8 mm)
- Sealing and reinforcement of sutures in pulmonary resections, lobectomies, pneumonectomies, bullectomies, volume reductions, tracheobronchial resections
- Vascular suture sealing during lung transplant procedures
- Hemostasis for oozing hemorrhages after dissections, decortications, pleural adhesions, tumors, and mediastinal masses
- Tracheal resection sealing and suture reinforcement
Clinical Evidence
- The nebulized application of Glubran® 2 in thoracic surgery has demonstrated significant clinical benefits:
- Prevention of air leaks: The incidence of early postoperative air leaks was 10.3% in the Glubran® 2 group versus 29.1% in controls (p<0.0001;
- Reduced chest tube duration: Average time with chest tube in place was 1.2 ± 0.3 days for Glubran® 2 patients versus 2.7 ± 1.1 days in the control group (p<0.0001)
- Shorter postoperative stay: Length of hospital stay was 2.4 ± 0.9 days compared to 3.8 ± 1.7 days in controls (p=0.03).
The use of nebulized Glubran® 2 also showed average savings of €750 per patient correlated with favorable clinical outcomes (Carlea F. et al., 2019).1
| OUTCOMES | STUDY GROUP (GLUBRAN® 2) N=192 | CONTROL GROUP N=192 | P VALUE |
|---|---|---|---|
| Early post-operative air leaks (incidence) | 10,3% | 29,1% | p<0,0001 |
| Chest Tube Drainage in Place (days) | 1,2±0,3 | 2,7±1,1 | p<0,0001 |
| Post-op length of stay (days) | 2,4±0,9 | 3,8±1,7 | P=0.03 |
Dedicated Devices
Spray devices are indicated for nebulized application in thoracic surgery:
- Apply a thin, elastic film of Glubran® 2 for aerostatic and hemostatic purposes
- Gas supply autonomy: 8 continuous minutes
- Coverage: 1 mL per 15×15 cm (225 cm²)
- Facilitates suture reinforcement and uniform sealing of the parenchyma
These results confirm that Glubran® 2 is effective, safe, and cost-efficient in thoracic procedures.
| DEVICE | IMAGE | DISTANCE FROM TISSUE | SPRAYING DIAMETER | INDICATIONS | THORACIC SURGERY |
|---|---|---|---|---|---|
| SPRAY DEVICE (G2-NBT) |
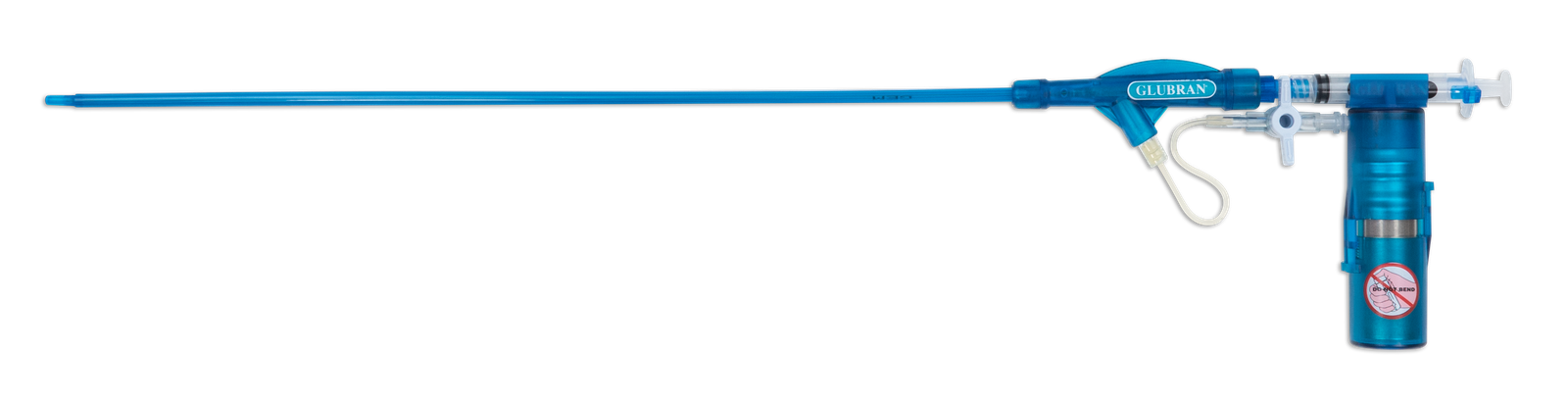
|
On large surfaces in thoracoscopy | Hemostasis and sealing of resections, decortications and bullectomies | ||
| RIGID SPRAY DEVICE (G2-NBT RIG) |
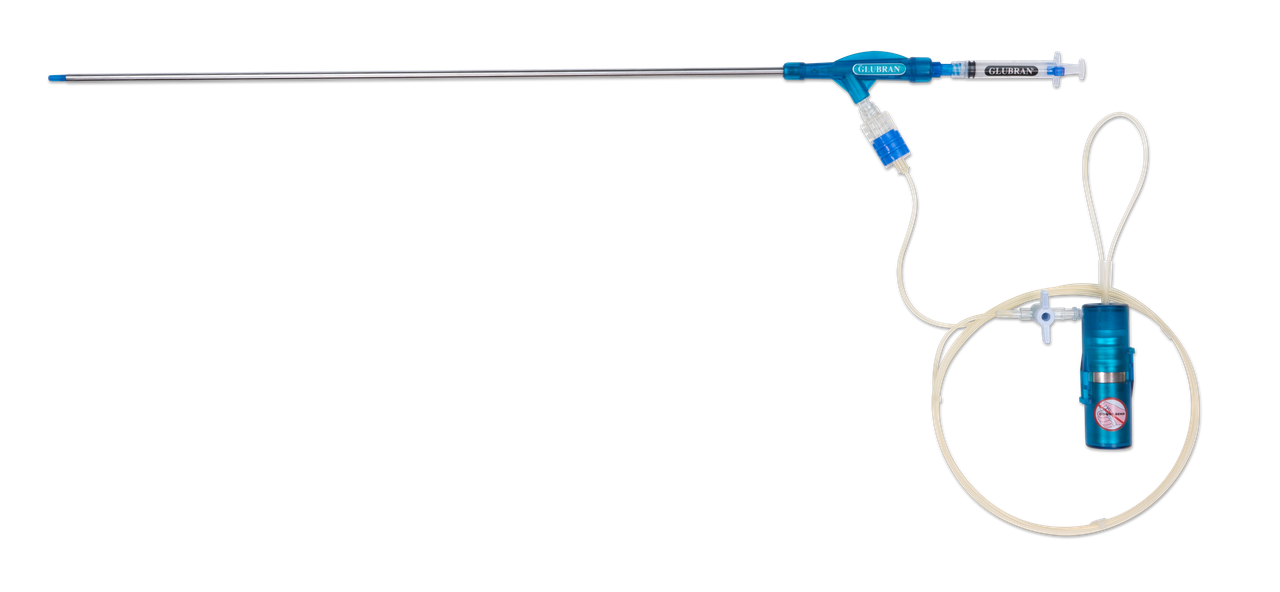
|
5–7 cm | 4 cm | ||
| SHORT SPRAY DEVICE (G2-NBT SHORT) |
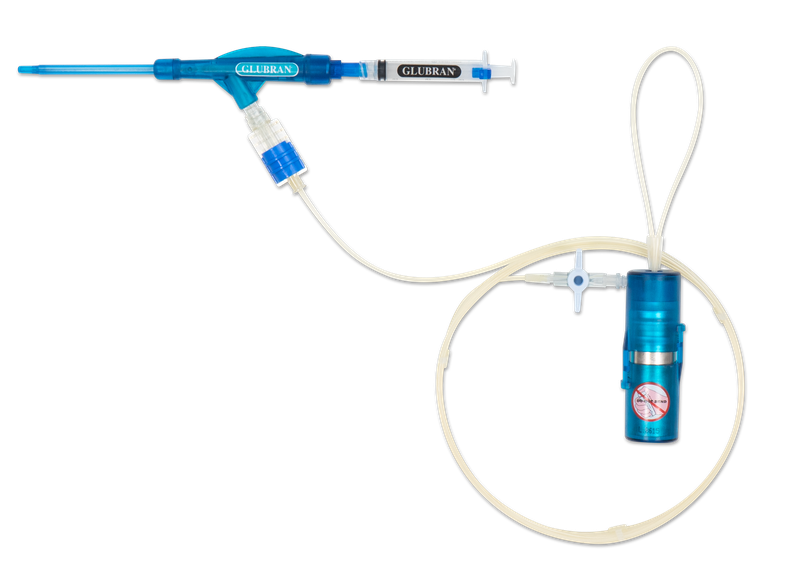
|
In open surgery | |||
| SMALL SPRAY DEVICE (G2-NBT SMALL) |
|
2–3 cm | 1 cm | For small surfaces in thoracoscopy |
Sealing and reinforcement of manual or mechanical suture lines. Hemostasis and sealing of biopsies |
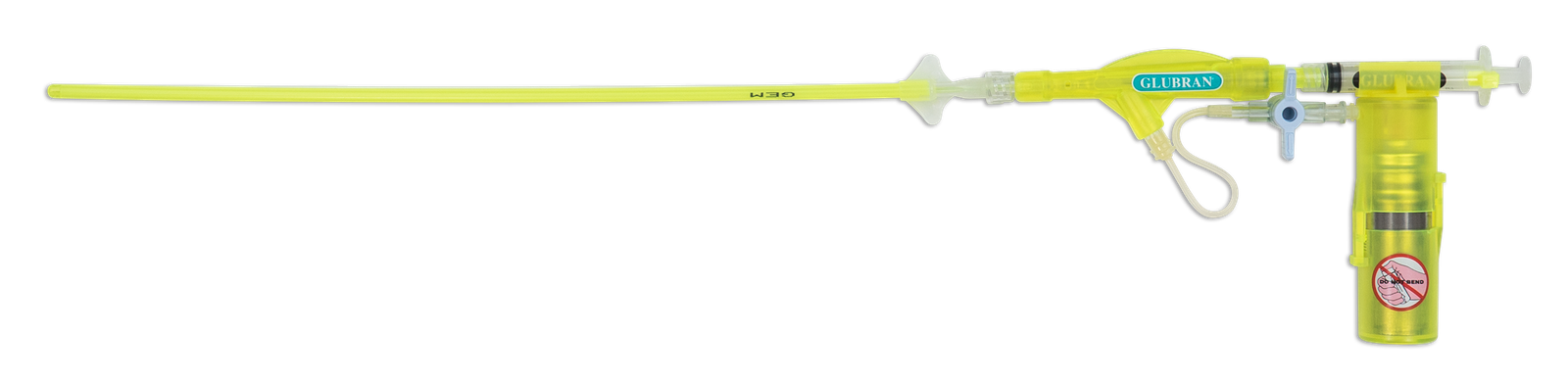
| SHORT MINI SPRAY DEVICE (G2-NBT SM SHORT) |
|
In open |
Usage Protocol
- Prepare the spray device and Glubran® 2 according to standard surgical procedures.
- Apply a thin, uniform layer over the target area using the nebulizer.
- Cover sutures, fistulas, or parenchymal surfaces completely for optimal aerostasis and hemostasis.
- Monitor the application to ensure complete coverage; 1 mL typically covers 225 cm².
- Proceed with routine surgical closure once adhesion is achieved.
The nebulized method ensures elastic, durable sealing without altering standard surgical workflow.
Bibliography
Carlea F. The Glubran®2 nebulizer for the prevention of air leaks. XLII SICO Congress, 2019.
Lozito C. Coating and reinforcement of sutures in oncological thoracic surgery. XXVIII SPIGC, 2017.
Alar T, et al. Prevention of prolonged air leaks after pulmonary lobectomy. Indian J Surg, 2013.
Pedicini V, et al. Pulmonary pseudoaneurysm treated with percutaneous coil and glue embolization. J Vasc Interv Radiol, 2017.
Lucernoni P, et al. Sarcoidosis case study. Rassegna di patologia dell’apparato respiratorio, 2003.
Gimferrer JM, et al. Video-assisted direct closure of bronchial fistula. J Laparoendosc Adv Surg Tech A, 2003.
García-Polo C, et al. Endoscopic sealing of bronchopleural fistulas with tissue expander. Can Respir J, 2010.
Saikia MK, et al. Bronchoesophageal fistula repair with NBCA glue. J Clin Diagn Res, 2016.
Davoli F, et al. Coagulant spray glue for aerostatic purposes in pigs. Eur Surg Res, 2009.
Mineo TC, et al. Nonintubated uniportal nonresectional videothoracoscopic lung volume reduction. Video-assist Thorac Surg, 2017.